 File this one under “Dr. Frankenstein’s Medicine Show.”
File this one under “Dr. Frankenstein’s Medicine Show.”
Let’s deal with the medicine part first and the Frankenstein part second.
On the medical front, good news! Researchers have found a way to communicate with patients who are in a “persistent vegetative state.”
Turns out that they, or some of them, ain’t so vegetable-like after all!
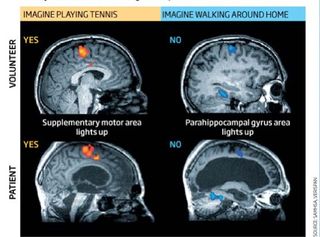
Here’s how it works: Hook the “vegetable” up to an MRI machine and ask the
vegetable
person to think about playing tennis. Note what areas of the brain light up.
Then ask the person to think about walking through their house. Note what areas light up then.
Then say, “I’d like to ask you some questions. If you want to answer ‘yes,’ think about playing tennis. If you want to answer ‘no,’ think about walking through their house. Do you understand?”
If the tennis-playing areas light up, go ahead and ask your questions. If the house-walking areas light up, explain again. (Or assume that the person is really smart and having a joke on you by thinking “no” when really he does understand.)
This really works!
At least with some patients. (Not with others, unfortunately.)
What it shows, though, is that these patients aren’t “vegetative” at all—at least mentally. They’re able to process and respond meaningfully to questions based on thinking about remembered/imagined actions.
That shows advanced cognitive functions! Remember: The person isn’t just thinking about saying “yes” or “no.” The person is thinking about other actions as a way of saying “yes” and “no.” That shows sophisticated mental processes in action!
So! Good news for the pro-life side, right?
Yesssss . . . but . . . here’s where Dr. Frankenstein—or at least Dr. Kevorkian—comes into the picture.
Already people are talking about using this technology to ask PVS patients questions like “Are you in pain?” and “Do you want to die?”
The first question is entirely legitimate! If someone’s in pain, let’s do what we can to alleviate it! By all means!
But let’s not proceed so quickly to the “Do you want to die?” question.
Other questions would be good ones, like “Do you need to change positions?”, “Are you hungry or thirsty?”, or “Would you like me to get a nurse?” or—once the immediate pain is dealt with—“Would you like me to get a priest to come pray with you and give you the sacraments?”, “May I squeeze your hand to show that I care about you?” (or even just do this one and don’t ask!), “Would you like me to turn the TV on?”, “Would you like to listen to some music?”, “How about an audio book? I could get you a subscription to Audible.com.” Or even, “Let’s use ‘yes’/‘no’ with the alphabet so you can tell me what you want. Think about what you’d most like, and we’ll spell it out.”
There are all kinds of compassionate alternatives to “Do you want to die?”
But folks are already noting that the new technique may put more pressure on people suffering from PVS to just go ahead and die.
So what can—and by rights should—be a vindication for pro-lifers may get twisted into a new way to promote euthanasia.
Hence: Dr. Frankenstein’s Medicine Show. . . . turning legitimate medicine to the service of evil.
Watch this one, folks. It’s going to be a BIG one as brain scanning technology becomes more common and more robust—allowing easier, richer communication with people in this state. It’ll be a major new feature of the discussion.
The work “changes everything”, says Nicholas Schiff, a neurologist at Weill Cornell Medical College in New York, who is carrying out similar work on patients with consciousness disorders. “Knowing that someone could persist in a state like this and not show evidence of the fact that they can answer yes/no questions should be extremely disturbing to our clinical practice.”
A comment posted at New Scientist (“Fri Feb 05 18:17:54 GMT 2010 by TheSimulacra”) seems to be saying that the article is actually not about people in the “vegetative state” (persistent or otherwise) or about people with “brain death”, but about people in a rare and different condition called “Locked-In Syndrome”. If so, then researchers have NOT “found a way to communicate with patients who are in a ‘persistent vegetative state'”. Rather, they’ve found a way to communicate with persons with “Locked-In Syndrome” (or some other condition). Indeed, to the extent that, by definition, “vegetative state” would necessarily mean that there is in fact an absence of awareness (i.e. “wakefulness without awareness”), there will never be any study showing that persons (truly) in a “vegetative state” have awareness. But there may be cases of misdiagnosis, such as due to faulty diagnostic criteria. As you said in your article, Jimmy, “What it shows… is that these patients aren’t ‘vegetative’ at all—at least mentally.”
Terry-
“Locked-In Syndrome” is what you call “persistent vegetative state” when they wake up or otherwise show that they’re not “vegetables.”
No, I don’t call “persistent vegetative state” “Locked-In Syndrome”, but maybe you do?
I think we need some definitions here. What is the real medical definition/understanding of “brain death”, “Persistent vegetative state” and “Locked-in Syndrome”? Any medical-type people who can tell us? I think understanding this is important. Look at Terri Schiavo’s case. The media insisted on caling her “brain dead” and in PVS, and so did her “husband”. But her family insisted she was not. If “brain death” and “PVS” mean that the person has no awareness, no response to anything, then, according to Terri’s family and the video that was posted to the Internet, she was NOT “brain dead” or in PVS. She recognized family, responded to them, made sounds and movements. Which the media did not report, as they seemed to be as set on having her killed as her “husband”, with the result that large numbers of people did not truly understand the situation and what the courts were being asked to decide. In the end, the courts made the decision to commit homocide by the slow starving to death of a person who was aware of her suffering. It’s possible that if there had been a clearer understanding of “brain death” and PVS, popular opinion, and maybe the courts’ decision, might have been different. I think the definition has a bearing on our understanding of the research Jimmy was talking about, too.
Actually, no. “Brain death” means the same thing to a real doctor that “death” meant to all humanity until a few decades ago, when what’s now called “clinical death” became something that people could recover from if doctors treated you quickly enough. When you “have” brain death, you are dead. A corpse. Ready to be buried. And entirely orthodox Catholic surgeons will feel no moral qualms whatsoever harvesting your organs for transplant.
The fact that irresponsible and often disingenuous reporters and euthanasia advocates blur the line between a person who is living with a severe neurological disability (such as PVS or “locked-in syndrome”) and a person who is already dead is unfortunate if rather predictable. But let’s not make the same mistake here.
At this time, it is not possible to employ the fMRI technique in any clinical way because the patient must be in the MRI while the questions are asked snd not only are the machines big, but there is usually only one in a hospital and it cannot be tied up. A much better technique may turn out to be magnetoencephalography which is more portable and can process faster brainfunctions.
The Chicken
http://www.firstthings.com/blogs/secondhandsmoke/2009/11/28/rom-houben-case-doctor-explains-how-he-knows-patient-is-conscious/
The above link from a good bioethics blog (defined as they try to figure out how to apply standard ethics instead of trying to figure out how to get around them) gives some insight on how people get put under the PVS label and never get out. Do a site-search for PVS and read the comments if you need to be depressed….
Laura,
In 1995 the American Academy of Neurology published a practice parameter about the assessment and management of patients in the persistent vegetative state, available here.
There is also the Wikipedia article.
In 1994, definitions for brain death, coma, locked-in syndrome, PVS and others were published here.
As defined, PVS does not exclude all responses, movements or sounds. For example, “They may move the trunk or limbs in meaningless ways. They may occasionally smile, and a few may even shed tears; some utter grunts or, on rare occasions, moan or scream.”
As defined, PVS does not exclude all responses, movements or sounds. For example, “They may move the trunk or limbs in meaningless ways. They may occasionally smile, and a few may even shed tears; some utter grunts or, on rare occasions, moan or scream.”
Sounds an awful lot to me like a definition crafted with the purpose of fitting as many people as possible under the “PVS” label – whether they have cognitive faculties or not.
In the US, we classify brain death as complete and irreversible death of the entire brain — from brainstem to cortex. It occurs after a severe brain injury which kills the brain. Because the heart has its own conduction system, it can beat for months despite a dead brain. In fact, the heart can even beat after being removed from the body. Breathing, however, depends on the brainstem. One of the tests we perform to determine brain death is the apnea test. The patient is disconnected from the ventilator, O2 is delivered directly in the lungs so the heart continues beating and internal organs remain alive, and we watch for any breathing movements for several minutes. The CO2 level will rise (a very potent stimulus for breathing). If the patient does not make *any* breathing movements despite a sufficiently elevated CO2, he/she failed the apnea test. If they also have no other signs of brain activity (pupils unreactive, eyes without any movement despite potent stimulus, no cough, no gag, etc.), then death is declared. A useful adjunct test measures blood flow into the brain. In these cases the brain has swollen within the skull such that no blood will enter it. If the patient were left on the ventilator, the brain would liquefy over a period of weeks.
Patients with PVS have preserved brainstem function. As stated above, they have periods of apparent sleep and wakefuless. They may respond to the environment, but only in a stereotyped way (e.g. they may turn to a sound, but will make the same movement to the same stimulus each time). To complicate things further, some neurologists define a “minimally conscious state” in which patients make more complex interactions with the environment.
Patients with locked in syndrome have very focal damage to an area of the brainstem called the pons (bridge). This prevents motor and sensation signals from passing through the pons. Only eye movements (whose 2nd order neurons originate from above the pons) can be made. These patients are fully awake. You can think of these patients as being very similar to a cervical spinal cord injury. Think of Christopher Reeve, but also unable to move their tongue, face, talk, etc.
Hope this helps.
Dear Martin,
You wrote:
Patients with PVS have preserved brainstem function. As stated above, they have periods of apparent sleep and wakefuless. They may respond to the environment, but only in a stereotyped way (e.g. they may turn to a sound, but will make the same movement to the same stimulus each time).
This is true, but in the case of Terry Schiavo, she laughed and it may have been oriented laughter. Unlike sterotypical auditory reflex reactions, laughter does not have such specific and repetitive triggers if it is only a brainstem response. In other words, there seems to be no cause and effect type of laughter for people in a PVS.
I have published peer-reviewed mathematical models of brainstem triggers in laughter and from what I can see (the models are very qualitative), gelastic seizures can occur if there is damage to the brainstem (hypothalamus, more specifically) causing a type of low frequency firing pattern similar to that triggered in the PFC (prefrontal cortex) during cognitive-mediated laughter. The problem in Schiavo’s case is that she had electrodes implanted in her thalamic region for deep brain stimulation and depending upon their placement, might be responsible for triggering gelastic seizures. The only way to know for certain if her laughter were incident to her brainstem injury (either due to oxygen deprivation or the electrodes) or if it were cognitively-mediated is by looking at an fMRI or MEG scan (EEG is not deep enough), which would have shown activation of the PFC if her laughter were cognitively-mediated.
This was not done. I have a colleague in Germany who fought for a patient whom everyone wanted to put away as being in a PVS, but he noticed that every time he went to visit the patient, when he playfully rolled up his pant leg, the patient started to laugh. My colleague managed to get the patient into rehab and he recovered.
I have toyed with the idea of trying to get laugher included as a diagnostic tool for PVS. I know many of the neuroscientists involved in the research of the neurobiology of laughter and I think they might be tempted to agree.
Schaivo may have been in a minimally conscious state. I don’t know how much activation current of the PFC is needed for mirthful laughter (there seems to be a type of high-low voltage switching that occurs), but there may have been enough cortical activity for this to occur. We will never know.
We really do know very little about the brain.
The Chicken
Chicken,
I agree. I was just trying to explain how clinicians look at brain death and why it’s a valid determination of legal death. The ventilator can be discontinued without ethical problems.
As far as PVS and minimally conscious state goes, I think we can agree that the patients are severely injured, but probably make up a heterogeneous mix. As far as the ethics go, we need to care for all these patients, regardless of extent of injury, as best we can.
I would be very interested if we could help identify PVS/MCS patients who may respond to PVS or other method of cognitive enhancement. BTW, I think someone has also published reports of intact long latency auditory evoked potentials in patients with PVS suggesting that *some* cortical processing is taking place. What this means for the individual patient (prognosis, possible treatment, etc), however, is unclear to me.
We really do know very little about the brain.
Amen. All the more reason to not decide to remove food and water from someone, true, but AMEN to the ^nth.
“They may move the trunk or limbs in meaningless ways.”
They do not know whether this movement is meaningless, or not.
“We really do know very little about the brain.”
Aye. The probems come when we behave as if we know more than we do.
My only objection to this new technique (or ones similar) is that, while they may be of some help in identifying cognitive activity, it should never become a test for identifying an absence of cognitive activity.
The most that could be said would be that a particular individual has no activity detectable by this technology.
Dear Tim J.
You wrote:
The most that could be said would be that a particular individual has no activity detectable by this technology.
Good point.
The Chicken